

A Child’s First Dental Visit
An exploration of why the age 1 visit is a game changer in terms of overall oral health and childhood caries.
PURCHASE COURSE
This course was published in the February 2019 issue and expires February 2022. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
The American Academy of Pediatrics, American Academy of Pediatric Dentistry (AAPD) and the American Dental Association recommend a child’s first dental visit take place at the eruption of the first tooth or by the child’s first birthday.1 Upon learning this, many parents and caregivers might initially think, “What! Age 1? What would you do on my 1-year old? She just started getting teeth recently!”
This course was published in the February 2019 issue and expires February 2022. The authors have no commercial conflicts of interest to disclose. This 2 credit hour self-study activity is electronically mediated.
EDUCATIONAL OBJECTIVES
After reading this course, the participant should be able to:
- Explain the concept and value of a dental home and the Age 1 dental visit, as well as utilization rates for this model of care.
- Describe fundamental clinical practices and challenges when caring for infants and young children.
- Detail key issues surrounding childhood caries and the need to educate parents and caregivers of young pediatric patients.
For the better part of the last 100 years, dentistry followed the “see and treat” concept; meaning that oral health care was, for the most part, treatment oriented. Dentists did what they were trained to do, which was to treat dental caries. Most patients visited the dentist to address a specific problem (usually prompted by the occurrence of pain). Many did not consider primary teeth important, since they were looked upon as being transitional, and would soon be exfoliated and replaced by permanent teeth. In fact, in the 1950s some dental offices had signs in their waiting rooms proclaiming, “No children under age 13 treated.”
With an increase in the knowledge of the dental caries process, dentists gradually began to see children at earlier ages. Many dentists were ill equipped to communicate with and/or treat such young patients; consequently, the recommended age for the child’s first dental visit was on or after the 3rd birthday. Dentistry for patients under the age of 3 was largely approached didactically and not clinically. Prevention of dental disease for this group was a mere afterthought.
PARADIGM SHIFT
Once dental caries was understood as a chronic bacterial disease with a behavioral component, the paradigm shifted from treating the resulting damage to addressing the cause (prevention). In turn, this shift had a significant impact on determining the optimal age for the first dental visit.
Dentistry will never “drill its way out” of the early childhood caries (ECC) epidemic. For practitioners to succeed in the fight against ECC, they must improve preventive efforts and manage lesions in their earliest stages. A patient’s risk of developing dental caries starts with the introduction of oral pathogens into an infant’s mouth; therefore, first seeing the dentist at age 3 could prove too late. The age 1 visit not only allows for preventive therapies and early treatment, it also benefits the child by helping to establish optimal feeding and oral hygiene habits.
In a 1992 policy statement, the American Academy of Pediatrics proposed a definition of the medical home and referred to the “delivery of advanced primary care, with the goal of addressing and integrating high quality health promotion, acute care, and chronic condition management in a planned, coordinated and family centered manner.”2 In 2001, the AAPD adopted its Policy on the Dental Home, based on the American Academy of Pediatrics’ medical home concept. Children who have a dental home are more likely to receive appropriate and routine preventive care and thus have a reduced risk of dental disease.3
The recommendation for a child’s first dental visit to occur at or before age 1 has been the standard since 2001. Yet, practically speaking, dentistry for patients under the age of 3 continues to be largely spoken of didactically, and not widely implemented clinically in general practice. This is not a criticism as much as an observation. Dentists are busy addressing the functional and physical effects of dental caries and have little time to address the process. Many have not been adequately trained to understand the purpose and method of introducing the age 1 patient to clinical practice. This article will explain the rationale, benefit and technique for implementing the age 1 dental visit. The goal is to make dental practitioners comfortable and competent in meeting this standard of care.
RATIONALE FOR EARLY CARE
Dental caries is a preventable, chronic disease that is influenced by social and behavioral factors. Improving access to — and the use of — preventive and disease management strategies, along with early dental visits, will contribute to better patient outcomes, reduction of per capita health care expenses, and improved utilization of services.
According to research, annual treatment costs for children who had their first dental visit by age 1 are significantly less than for patients who wait until they are older.4 Children seen by a dentist before age 1 are more likely to see the dentist on an ongoing basis, and less likely to require restorative or emergency visits. By comparison, those seen for the first time at age 2 and age 3 have an increased need for preventive, restorative and emergency visits over time.5
Unfortunately, 23% of children continue to experience dental caries, with children from ages 2 to 5 experiencing increasing rates.6 In 2015, 57% of children on Medicaid did not receive preventive oral health services.7 Previous research showed that Medicaid patients ages 1 to 5 accounted for 45% of total dental costs, even though this age group represented only 5% of the insured population.6 In a 2015 retrospective review of privately insured patients, only 1% had their first dental visit by age 1.8
It is logical to ask, “If so much could be done to enhance oral health with effective preventive strategies implemented in the first year of life, why hasn’t dentistry been more effective in this regard?” This is a good question with a complex answer.
Seldom is a patient under the age of 3 cooperative in the dental office. If the dentist’s role is only restorative, there is a dilemma of how to perform complicated procedures on kicking, screaming and crying patients. In years past, many dentists were ill prepared to cope with such patients, therefore treatment was delayed until after the patients were better able to cooperate, usually after their 3rd birthday.
Only recently have the age 1 visit, the value of a dental home, and the clinical skills to complete an infant oral examination been emphasized in dental school curricula. While practicing general dentists may have been exposed to these concepts, as previously noted, many have not been trained in the delivery of care for such young patients.
In addition, dentists are trained to diagnose and restore the consequences of dental disease. Far too often, dentistry is viewed as a surgical specialty, and the schedules of many dentists are customarily filled with patients having broken-down teeth needing immediate attention. If this pattern is to be reversed, there must be a complete paradigm shift emphasizing preventive care and, when possible, nonsurgical management.
This emphasis on early dental visits and subsequent recall appointments (i.e., the dental home) is grounded in risk analysis, as well as education and guidance directed toward parents and caregivers. In short, the anticipatory guidance provided is of primary value.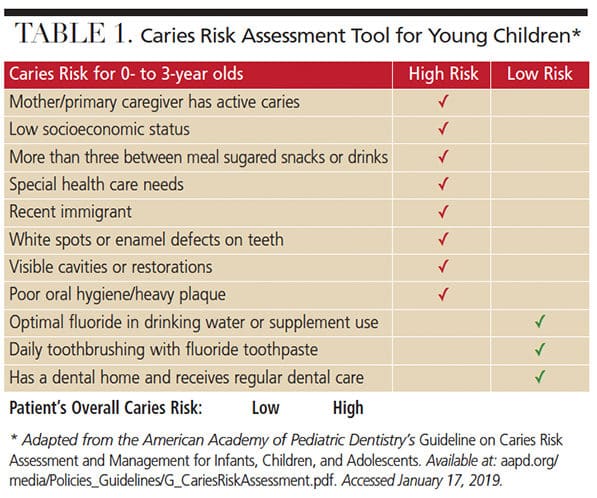
THE THREE PILLARS
A proper infant oral examination visit rests upon three pillars:
- Risk assessment
- Oral examination
- Anticipatory guidance
Risk Assessment: Effective infant preventive dentistry begins with an assessment of individual risk factors, as established through the medical, social and dental histories (Table 1). Preventive strategies are subsequently developed to address the patient’s specific risk. These activities occur before the patient’s oral exam and are aimed at providing the primary caregiver with adequate information to reduce the risk of dental caries.
Special attention should be given to the primary caregiver’s dental history. The infant’s oral pathogens are the result of vertical transmission from the primary caregiver. Untreated caries and high bacterial counts from periodontal conditions in the caregiver’s mouth result in the infant having a bacterial flora conducive to caries development.9

Feeding habits affect caries risk through both what is eaten, and how it is eaten. Carbohydrate-rich diets are highly cariogenic and should be limited. Feeding on demand and/or at night leads to what was formerly referred to as “baby bottle decay,” but now is now known as ECC.10 The American Academy of Pediatrics recommend infants be breastfed until age 1.11 Breastfeeding or bottle-feeding should not be ad lib. Feeding at night increases the risk of caries formation. During sleep, the body’s systems slow and respirations and the heart rate decreases. There is also reduced salivary flow, and this diminishes the natural cleaning and buffering effect of saliva.
Oral Examination: The examination of the infant’s oral cavity takes place in a knee-to-knee fashion (Figure 1). The dentist cradles the infant’s head in his or her lap while supporting the head. The caregiver holds the infant’s hands and feet. It is normal and beneficial for the infant to cry, as this ensures the mouth is open and an adequate visual examination is possible. The dentist should communicate throughout the examination and remain complimentary of the infant and caregiver. Clinical observations should be pointed out, and the provider should demonstrate proper technique for cleaning the teeth using a gauze, toothbrush or washcloth. Finally, fluoride varnish should be applied. (Additional clinical resources are found in Table 2.)
Anticipatory Guidance: In terms of diet and feeding habits, breastfeeding should be encouraged and added carbohydrates avoided. Feeding should be on a schedule and infants should never be put to bed with a bottle. Water after feeding should also be encouraged.
The child should be introduced to toothbrushing when the first tooth erupts. A soft-bristle brush with an age-appropriate amount of fluoridated toothpaste is recommended (refer to the AAPD’s guideline on fluoride use). As noted, the dentist should demonstrate the technique to the caregiver during the knee-to-knee examination. Other sources of fluoride include drinking fluoridated water and use of fluoride varnish, which should be placed on primary teeth at each dental visit.
TOOTH ERUPTION
A discussion of tooth eruption (including any anticipated eruption problems) and teething should be covered during the visit. Special instruction should be given to avoid over-the-counter numbing gels because of the risk of toxicity; however, over-the-counter pain medications can be given.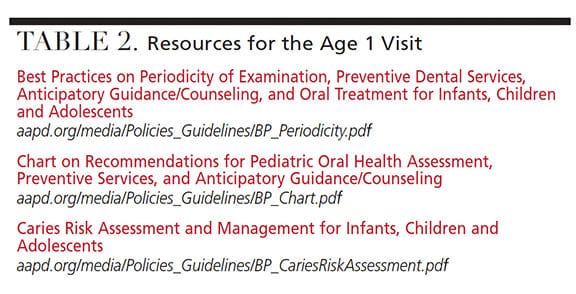
NONNUTRITIVE HABITS
Nonnutritive oral habits are common in infants. The caregiver should be assured these are normal and that most infants discontinue them in time. Persistent habits that are causing distortion of the oral cavity can be addressed when the patient is mature enough to want to quit. Until then, the dentist should monitor the habit and any resulting oral changes it is causing.
RECALL VISITS
High-risk patients should be placed on a three-month recall schedule. Fluoride varnish should be applied at these visits. Additional anticipatory guidance information should be reemphasized at each appointment. More information on the infant examination can be found in the AAPD Guideline for Infant Oral Health Care (aapd.org/ media/ Policies_ Guidelines/ G_ InfantOralHealthCare.pdf).
CONCLUSION
Dentists who provide care for pediatric patients are highly encouraged to adopt the age 1 visit. It is the standard of care for young patients and supported by the AAPD, American Dental Association and American Academy of Pediatrics. While preventive measures are important for all patients, waiting to institute these measures at age 3 would be too late for patients at high risk of dental caries. The patient with ECC will require more dental care, incur more expense, and is likely to face a lifetime of caries. For dentistry to address this dilemma in any significant way requires intervention upon the eruption of the first primary tooth.
Just as pediatricians are the primary medical care providers for infants, dentists are the primary oral health care providers for this patient population. The role and responsibility of the dentist is to provide education and training to the parents/caregivers and, when appropriate, the child, too. The value of the child’s first dental visit, and subsequent routine appointments, is not merely the dental prophylaxis. It is the supervision and educational information the parent/caregiver and patient receives from the dental team that will provide a lifetime of value in terms of oral and overall health.
REFERENCES
- American Academy of Pediatrics. Maintaining and improving the oral health of young children. Section on oral health. Pediatrics. 2014;134:1224–1229.
- American Academy of Pediatrics. Medical Home definition. Available at: https://www.aap.org/en-us/professional-resources/practice-transformation/ medicalhome/Pages/home.aspx. Accessed January 17, 2019.
- American Academy of Pediatric Dentistry. Definition of Dental Home. Available at: http://www.aapd.org/ media/policies_guidelines/d_dentalhome.pdf. Accessed January 17, 2019.
- Dye BA, Thornton-Evans G, Li X, Iafolla TJ. Dental caries and sealant prevalence in children and adolescents in the United States, 2011–2012. NCHS Data Brief. 2015;191:1–8.
- Nowak A, Christensen JR, Mabry TR, Townsend JA, Wells MH. Pediatric Dentistry: Infancy through Adolescence. 6th ed. Philidelphia: Saunders; 2018:137.6.
- Lee JY, Bouwens TJ, Savage MF, Vann WF Jr. Examining the cost-effectiveness of early dental visits. Pediatr Dent. 2006;28:102–105.
- Casamassimo PS, Hammersmith K, Gross EL, Amini H. Infant oral health: an emerging dental public health measure. Dent Clin North Am. 2018;62:235–244.
- Kolstad C, Zavras A, Yoon RK. Cost-benefit analysis of the age one dental visit for the privately insured. Pediatr Dent. 2015;37:376–380.
- Dye BA, Vargas CM, Lee JJ, Magder L, Tinanoff N. Assessing the relationship between children’s oral health status and that of their mothers. J Am Dent Assoc. 2011;142:173–183.
- Kierce EA, Rainchuso L. Comprehensive approach to early childhood caries. Decisions in Dentistry. 2017;3(12):34–36,39.
- The American Academy of Pediatrics Policy on Breastfeeding. Available at: https://www.aap.org/en-us/advocacy-and-policy/aap-health-initiatives/ Breastfeeding/Pages/AAP-Policy-on-Breastfeeding.aspx. Accessed January 17, 2019.
Featured image by ONDROOO/ISTOCK/GETTY IMAGES PLUS
From Decisions in Dentistry. February 2019;5(2):30—32,35.


Brushing is should start as soon as teeth appear, which can be as early as 4 months. Babies usually get bottom teeth first, then top ones. Don’t get too worked up about when baby teeth come in.